Over the past decade, the treatment landscape for mood and anxiety disorders has expanded significantly with the emergence of interventional modalities, most notably ketamine-based therapies and transcranial magnetic stimulation (TMS). These interventions have provided clinically meaningful benefit for patients with treatment-resistant conditions and have addressed longstanding gaps in therapeutic efficacy.
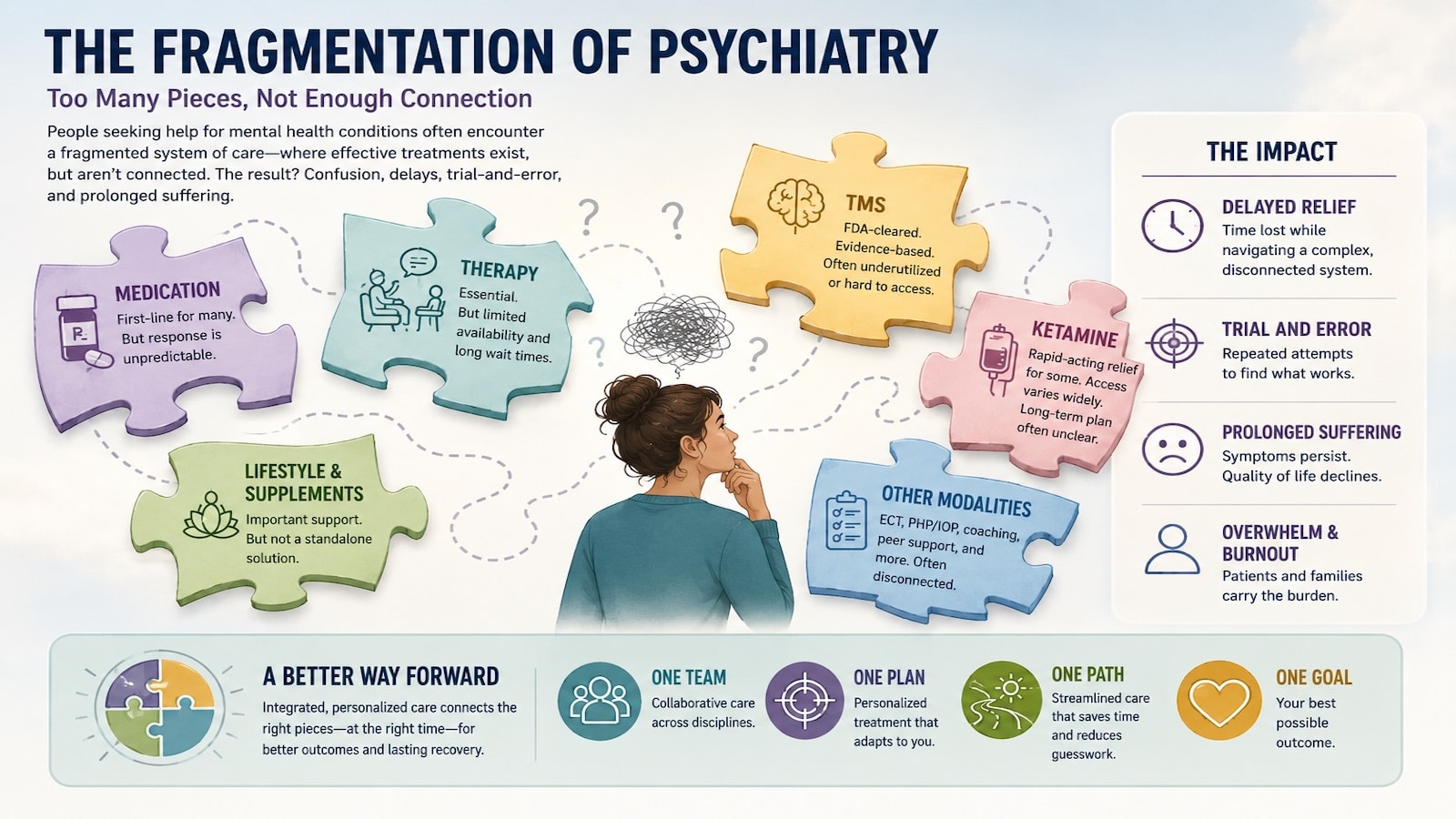
Concurrently, the rapid proliferation of specialized ketamine and TMS clinics has introduced new structural dynamics into outpatient psychiatric care. While these developments have improved access to novel treatments, they have also contributed to an increasingly fragmented care environment. Fragmentation is defined as the distribution of care across multiple providers without systematic coordination and represents an underexamined consequence of this evolving model.
In this article, we examine the structural drivers of fragmentation in interventional psychiatry and explore practical approaches to improving coordination across providers, particularly within regional referral networks such as the Washington, DC area.
Structural Drivers of Fragmentation in Interventional Psychiatry
The emergence of fragmentation in interventional psychiatry reflects broader structural forces rather than deficiencies at the level of individual clinicians.
Outpatient psychiatry remains constrained by limited clinician availability and increasing demand, restricting the ability of individual psychiatrists to incorporate resource-intensive interventional treatments into routine practice. At the same time, the rapid adoption of ketamine and TMS has outpaced traditional training pathways, resulting in reliance on external, specialized clinics for treatment delivery.
These interventions require distinct operational infrastructures—including nursing support, monitoring protocols, and device-based workflows—that differ substantially from standard outpatient care. This has incentivized the development of modality-specific centers designed for efficiency and scalability.
Market forces have further reinforced this structure, prioritizing access to high-demand treatments through specialized service lines rather than integrated care models.
Training Gaps and the Separation of Care in Psychiatric Training
An additional and often underrecognized driver of fragmentation lies in the structure of psychiatric training.
For many years, exposure to interventional treatments such as TMS—and more recently ketamine—has been limited or absent within standard residency curricula. As a result, many practicing psychiatrists have had minimal formal training in these modalities and may feel less comfortable incorporating them directly into their own practices.
This has contributed to a natural division of labor:
- General psychiatrists maintain responsibility for diagnosis and medication management
- Specialized clinics assume responsibility for interventional treatment delivery
While this division has facilitated access, it has also reinforced fragmentation by separating treatment modalities from the longitudinal care framework in which they are ideally embedded.
The anticipated introduction of psychedelic-assisted therapies is likely to further widen this gap. These treatments involve distinct therapeutic models, certification pathways, and delivery structures that may reside outside traditional psychiatric training environments.
Without deliberate incorporation into training programs, future psychiatrists may similarly rely on external centers for these interventions, perpetuating a distributed, and potentially fragmented, model of care.
The Future of Psychiatric Practice: Reintegrating Interventional Care in DC Healthcare
An important consideration in addressing fragmentation lies in the evolution of psychiatric training and scope of practice.
As exposure to interventional modalities, such as ketamine and TMS, becomes more integrated into residency and fellowship training, future psychiatrists are likely to develop greater familiarity with these treatments—not only in terms of indications, but also in dosing strategies, treatment sequencing, and maintenance planning.
This shift has the potential to alter the current division of labor in which interventional treatments are frequently outsourced to specialized clinics. With appropriate training, psychiatrists may increasingly assume a more direct role in guiding these aspects of care, including:
- Determination of appropriate candidates for interventional treatment
- Individualization of dosing protocols and treatment parameters
- Longitudinal planning for maintenance and relapse prevention
- Integration of interventional response into broader treatment strategies
Importantly, this evolution does not obviate the need for specialized infrastructure. Interventional treatments will continue to require clinical settings with appropriate monitoring, staffing, and safety protocols. However, the locus of clinical decision-making may shift toward the treating psychiatrist, even when procedural components are delivered within dedicated environments.
Such a model would preserve the operational advantages of specialized centers while restoring continuity of care through psychiatrist-led clinical oversight.
Clinical Manifestations of Fragmentation
In clinical practice, fragmentation is reflected in the separation of core components of psychiatric care:
- Longitudinal medication management
- Psychotherapeutic intervention
- Interventional treatment delivery
These elements are frequently distributed across multiple providers operating within distinct clinical frameworks and documentation systems.
While each component may be delivered with high quality, the absence of structured coordination introduces several challenges:
- Discontinuity in clinical formulation
- Delayed integration of treatment response into medication strategies
- Ambiguity in longitudinal responsibility for care
- Increased vulnerability during transitions following treatment completion
These issues reflect systemic limitations in communication and coordination rather than deficiencies in individual care.
The Next Wave: Psychedelic Therapies and the Risk of Further Fragmentation
The near-term introduction of additional psychedelic therapies, most notably MDMA-assisted therapy and psilocybin-based interventions, has the potential to further reshape the care landscape.
These treatments introduce additional complexity through:
- Distinct therapeutic frameworks
- New certification and training pathways
- Emergence of dedicated treatment centers
- Further separation of care components
Absent intentional integration, these developments may amplify existing fragmentation and introduce additional discontinuities in care.
A Proposed Model: Integrated, Psychiatrist-Led Interventional Care in Washington, DC
A potential path forward involves the development of care models that preserve access to advanced treatments while restoring continuity and coordination.
Key elements include:
- Centralized psychiatric oversight
- Interventional treatments embedded within broader care frameworks
- Structured communication protocols across providers
- Defined transition pathways following treatment
- Integration of interventional modalities into training
- Measurement-based longitudinal tracking
In our Washington, DC–based practice, this model is implemented through direct communication with referring clinicians, structured updates during treatment, and clear transition planning following completion of interventional care. Treating psychiatrists remains central to longitudinal management, while interventional treatments are delivered within a coordinated framework.
Conclusion
The field of psychiatry is entering a period of rapid therapeutic expansion.
Ketamine and TMS have already altered the treatment landscape, and the introduction of psychedelic therapies is likely to accelerate this transformation. At the same time, gaps in training and system design have contributed to an increasingly fragmented model of care.
The central challenge moving forward will not be access alone, but integration.
Ensuring continuity, coordination, and shared clinical responsibility will be essential to translating short-term therapeutic gains into sustained, long-term outcomes.
As interventional psychiatry evolves, models that prioritize collaboration between treating psychiatrists, therapists, and interventional providers will be essential. We continue to explore ways to strengthen these partnerships in clinical practice within the Washington, DC area.
For clinicians considering where to refer their patients to, the ability to maintain continuity while incorporating interventional treatments is critical. Structured collaboration between treating psychiatrists and interventional providers can help ensure that short-term gains translate into sustained clinical improvement. We are always available to discuss potential cases or provide guidance on whether a patient may be an appropriate candidate for TMS or ketamine therapy. Additional information on the referral process is available on our referral page.

